


Safe Gallbladder Surgery – My personal views
1st July 2022
Laparoscopic cholecystectomy (LC) or keyhole surgery removing the gallbladder was first done in Singapore in 1990. My own experience in this procedure started in the early 2000s.
There are lots of surgical literature regarding the safety and techniques of gallbladder surgery. Recently there is also a trend to publish classifications of cholecystitis (infected gallbladder).
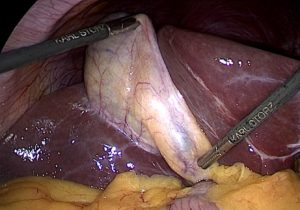
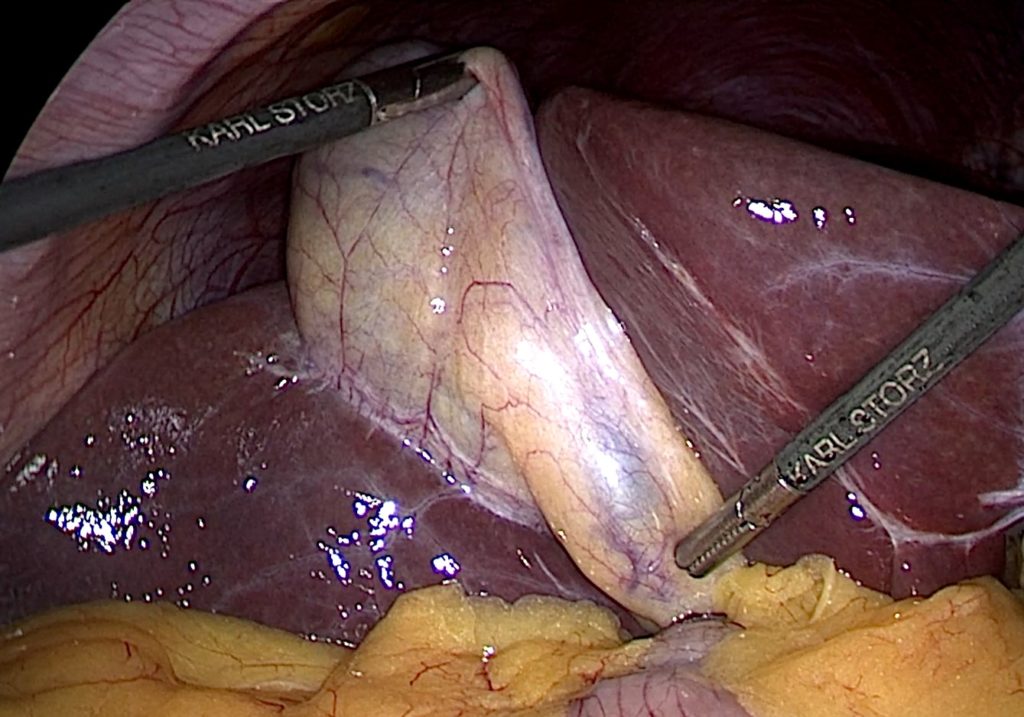
Current teaching in laparoscopic cholecystectomy stresses on the dissection of Calot’s triangle, in the process of displaying the cystic duct and cystic artery.
Calot’s triangle is bounded by the liver, common hepatic duct and the cystic duct. This is a modification of Calot’s original description in 1891 which was the cystic duct, common hepatic duct and the cystic artery.
I believe Calot’s dissection started from the side of the common hepatic duct. In the process, the artery is separated from the cystic duct and hence the triangle is identified. Current teaching does not encourage the dissection from the common hepatic duct. I personally will start just below the Hartmann’s pouch and cystic duct junction.
I have come across many surgical trainees or even surgeons doing laparoscopic cholecystectomy who will dive straight into finding Calot’s triangle.
Being mindful of the following components will lead to a good laparoscopic cholecystectomy (removal of gallbladder)
a) The scans – Always look at the ultrasound or CT/MRI scans of the gallbladder and the biliary tree. Contracted or shrunken gallbladders tend to be more challenging then a dilated one. Keep an eye on the insertion of the cystic duct into the common bile duct.
b) Mobilising Hartmann’s pouch – This will allow a safer dissection of Calot’s triangle. This step does improve the ease of identifying the cystic duct and arterial branches.
c) Anterior and posterior cystic artery anatomy is variable – Textbooks and traditional teaching is to identify the cystic artery. In my experience, it is common to find an anterior as well as a posterior branch. Consciously looking for both branches reduces the risk of unexpected bleeding.
d) Ensuring no stones remains in cystic duct – This is especially true in acute cholecystitis (infected gallbladder). Leaving stones behind in the cystic duct can cause long term problems and treatment can be rather complicated.
e) Safe control of cystic duct stump – Using plastic or metal clips. In complicated cases, ties or suturing.
f) Subtotal cholecystectomy – Able to decide when to leave the posterior wall of the gallbladder behind and when to leave a small portion of Hartmann’s pouch. This is not routinely done but a useful technique in complicated cases.
This blog may be a little too medical and technical. However, these are simple but significant steps which will help with a difficult “HOT” gallbladder. (Hot gallbladder is a term commonly used by surgeons to describe an infected gallbladder)
WW
Share this blog via:
- ← Health Screening – Raised Cancer Markers CEA, Ca 19-9 and aFP
- Unusual complications of gallstone – Case 1 →